
We specialise in every approach — so the right one is always available to you.
There is no single rhinoplasty technique that suits every patient. Whether you are researching preservation rhinoplasty, weighing open versus closed rhinoplasty, or exploring options for a specific concern — hump reduction, tip refinement, ethnic rhinoplasty, or a revision after a previous surgery — Dr. Buonassisi performs all of them, and selects the approach that is right for your anatomy.
Understanding the techniques available — and how they differ — helps you arrive at your rhinoplasty consultation with better questions and clearer expectations. The entries below describe each approach on its own terms, but the surgical plan is always considered as a whole: most results require several complementary changes working together.
The technique is never chosen in advance. It is recommended after Dr. Buonassisi has assessed your nasal anatomy, skin thickness, cartilage strength, and the specific changes you want to achieve. Patients come to 8 West from across Vancouver, North Vancouver, and the broader Lower Mainland — as well as from Victoria, Kelowna, Calgary, and internationally.
Most patients come to this page with one specific concern in mind — a bump, a tip that lacks definition, a nose that feels out of proportion. The techniques below will help you understand what is actually involved in addressing that concern, and why the surgical plan almost always extends beyond a single isolated change. That context makes for a more productive consultation.
Every approach. One goal: a result that looks like you.
The techniques below describe the approaches Dr. Buonassisi uses — but it is important to understand that rhinoplasty is rarely a single isolated change. A nose that looks natural is almost always the result of several small adjustments working together. Reducing a dorsal hump, for example, nearly always requires addressing the tip at the same time: a hump reduction that leaves the tip untouched tends to look unbalanced, because the proportions of the nose have shifted without the tip being brought into harmony.
What patients often describe as a single concern — “I just want my bump reduced” or “I just want my tip refined” — usually involves a series of complementary manoeuvres to achieve a result that looks like it was always there. Dr. Buonassisi will explain exactly what is involved for your anatomy at consultation. The entries below describe each technique on its own terms, but the surgical plan is always considered as a whole.
Hump Reduction Rhinoplasty
Smoothing the nasal bridge for a refined, balanced profile.
A dorsal hump is a prominence of bone and cartilage along the nasal bridge. Hump reduction lowers this profile line — either by excising the excess tissue (traditional approach) or by letting down the dorsum while preserving the native anatomy (preservation approach). The result is a straighter, more refined bridge that harmonises with the rest of the face.
A prominent nasal hump can dominate the profile and draw attention away from the eyes and lips. Reducing it restores facial balance — often with a dramatic improvement in the overall profile. It is worth noting that hump reduction in isolation is rarely the complete picture: lowering the bridge changes the proportions of the nose, and the tip almost always needs to be addressed at the same time to maintain harmony. A reduced bridge with an unchanged tip can look disproportionate.
Patients with a visible dorsal hump on profile view. In the vast majority of cases, hump reduction is planned alongside tip work — the two changes are considered together to ensure the result looks balanced from every angle, not just in profile.
Dr. Buonassisi evaluates the hump's composition (bone, cartilage, or both), the strength of the middle vault, and the patient's skin thickness. He determines whether a preservation let-down or traditional resection is more appropriate, whether osteotomies or spreader grafts are needed to close the roof, and what tip work — if any — is required to keep the nose in proportion after the bridge is lowered.
Preservation Rhinoplasty
The most significant advance in rhinoplasty in the past decade — conserving what works, refining what doesn't.
Rather than removing and rebuilding nasal structures, preservation rhinoplasty conserves the natural ligaments, cartilage, and periosteum. The dorsum is lowered by letting it down rather than cutting it away. This keeps the native anatomy intact and produces results that look and feel natural — because they largely are.
Traditional rhinoplasty involves significant disruption of nasal anatomy. Preservation rhinoplasty avoids this, resulting in less swelling, a faster recovery, a lower revision rate, and results that age more gracefully. As with all rhinoplasty, the technique addresses the nose as a whole — the dorsum and the tip are considered together, not in isolation.
Patients seeking hump reduction who have a good nasal tip and adequate skin quality. Not every anatomy is suitable — the technique requires a specific nasal structure to work correctly. Dr. Buonassisi is one of a small number of surgeons in Canada offering this approach.
Candidacy is assessed at consultation. Dr. Buonassisi evaluates the height and composition of the dorsal hump, the strength of the middle vault, and the relationship between the dorsum and the tip. The tip is always considered as part of the plan — preservation rhinoplasty is not simply a bridge procedure.
Tip Refinement & Rotation
Reshaping the nasal tip for improved definition, projection, and proportion.
Tip rhinoplasty involves reshaping the lower lateral cartilages that form the tip and alar rims. Techniques include cephalic trim (removing a measured strip of cartilage), tip sutures (transdomal, interdomal), columellar strut grafts, and tip rotation manoeuvres — used in combination based on the anatomy.
The tip is the most visible and defining part of the nose. A bulbous, drooping, or poorly projected tip can affect the overall harmony of the face even when the bridge is straight. Tip work is rarely a single manoeuvre — a natural result typically requires several small adjustments working together, calibrated to the specific anatomy and the changes being made elsewhere on the nose.
Patients concerned with the shape, definition, or position of their nasal tip. Tip work is frequently performed alongside bridge work — the two areas are closely related, and changes to one affect the perceived proportions of the other. Patients with thick skin should have a realistic conversation about the degree of definition achievable.
Dr. Buonassisi assesses cartilage strength, skin thickness, and the specific nature of the tip concern. He uses the most conservative combination of manoeuvres that achieves the desired result — always considering how the tip will read in proportion to the rest of the nose after all planned changes are made.
Open Rhinoplasty
Full surgical access for complex cases, significant tip work, and revision surgery.
Open rhinoplasty uses a small incision at the base of the columella — the strip of tissue between the nostrils — to lift the skin and expose the full nasal framework. This gives the surgeon complete visibility of all nasal structures: the tip cartilages, the dorsum, the septum, and the nasal bones.
Many rhinoplasty goals require precise work across multiple areas of the nose — tip, bridge, and septum — that simply cannot be done accurately through a closed approach. The open approach makes complex, multi-area work possible with the precision required to achieve a natural result. The columellar scar is discreet and typically fades to near-invisibility within 12 months.
Patients requiring significant tip work, complex structural changes, or revision surgery. Also preferred when cartilage grafts need to be placed with precision, or when multiple areas of the nose are being addressed in a single procedure.
Dr. Buonassisi uses the open approach when the complexity of the planned changes requires it. This is determined at consultation after assessing the full scope of what needs to be done — not just one area in isolation.
Closed Rhinoplasty
All incisions inside the nostrils — no external scarring, slightly faster recovery.
Closed rhinoplasty places all incisions inside the nostrils, leaving no visible external scar. The surgeon works through these internal incisions to access and reshape the nasal structures. The technique limits the degree of exposure compared to open rhinoplasty, which constrains what can be achieved.
For patients requiring more limited changes — particularly bridge work where the tip does not need significant restructuring — closed rhinoplasty can achieve excellent results with no external scar and a slightly shorter recovery. It is not a lesser technique; it is simply appropriate for a different scope of work.
Patients requiring limited changes, particularly to the bridge or dorsum, where the tip is already in good proportion and does not need significant modification. Not every anatomy is suitable — Dr. Buonassisi will advise whether the closed approach can achieve your goals without compromising the overall result.
The decision between open and closed rhinoplasty is made at consultation based on the full scope of changes required. If the planned work is limited enough that full exposure is not needed, closed rhinoplasty is a good option. If multiple areas need to be addressed together, the open approach is usually more appropriate.
Ethnic Rhinoplasty
Enhancing your features while preserving the characteristics that define your heritage.
Ethnic rhinoplasty refers to rhinoplasty performed with an explicit commitment to preserving the patient's ethnic characteristics. It is not a single technique — it is an approach and a philosophy. The anatomical considerations vary significantly across different ethnic backgrounds, and the goals are always defined by the patient.
Rhinoplasty that ignores ethnic anatomy can produce results that look operated-on, that erase cultural identity, or that create structural problems. Dr. Buonassisi's approach is to enhance harmony within the patient's own aesthetic framework — not to impose an external standard. As with all rhinoplasty, the nose is considered as a whole: changes to one area are always assessed in the context of the full face.
Patients of any background who want to improve the appearance of their nose while retaining the characteristics that reflect their heritage. Dr. Buonassisi has extensive experience with patients of East Asian, South Asian, Middle Eastern, African, and Latin American backgrounds.
The consultation focuses on understanding what the patient wants to preserve as much as what they want to change. Dr. Buonassisi assesses the specific anatomical characteristics — skin thickness, cartilage strength, tip anatomy, alar base width — and plans a series of complementary changes that work together to achieve a natural, harmonious result.
Revision Rhinoplasty
Correcting unsatisfactory results from a previous rhinoplasty.
Revision rhinoplasty addresses the aesthetic or functional problems that have resulted from a previous procedure. It may involve correcting over-resection, asymmetry, collapse, scarring, or an unnatural appearance. Cartilage grafts — often from the ear or rib — are frequently required to rebuild structure that was removed or damaged.
Many revision cases are the result of a previous procedure that addressed one area of the nose without considering the whole. A bridge that was reduced without corresponding tip work, or a tip that was over-refined without accounting for long-term structural integrity, are common examples. Revision rhinoplasty corrects these imbalances — but it is among the most technically demanding operations in facial plastic surgery.
Patients who are unhappy with the results of a previous rhinoplasty — whether performed elsewhere or at 8 West. Common concerns include a pinched tip, an over-reduced bridge, breathing problems, asymmetry, or a result that looks operated-on. A minimum of 12 months should have passed since the previous surgery.
Dr. Buonassisi begins with a thorough assessment of the existing anatomy, the previous surgical record if available, and the patient's specific concerns. He explains what is achievable in a revision setting — which is often more limited than a primary rhinoplasty — and sets realistic expectations before any plan is made.
Facial Feminization — Rhinoplasty
Subtle nasal refinements as part of a comprehensive facial feminization approach.
Rhinoplasty as part of facial feminization surgery (FFS) typically involves tip refinement, bridge narrowing, and upward rotation of the tip — manoeuvres that soften masculine nasal features and create a more feminine profile. The changes are calibrated to harmonise with other feminization procedures being performed.
The nose is a central feature of the face and a significant contributor to perceived gender. Subtle changes — particularly to the tip and bridge — can have a meaningful impact on overall facial femininity without looking surgical.
Patients undergoing facial feminization surgery who want to address the nose as part of a broader facial harmony plan. Can also be performed as a standalone procedure. Dr. Buonassisi works with each patient to understand their goals and the degree of change they are seeking.
The rhinoplasty plan is developed in the context of the full FFS plan — considering the forehead, jaw, and chin work being performed alongside it. Dr. Buonassisi assesses the nasal anatomy and recommends the specific manoeuvres that will achieve the most harmonious result.
Septoplasty
Correcting a deviated septum to restore natural airflow — often combined with cosmetic rhinoplasty.
Septoplasty straightens the nasal septum — the cartilage and bone that divides the nasal cavity. A deviated septum can obstruct airflow on one or both sides, causing chronic nasal congestion, mouth breathing, and sleep disruption. The procedure is performed through internal incisions with no external scarring.
Many patients seeking cosmetic rhinoplasty also have a deviated septum that affects their breathing. Combining septoplasty with rhinoplasty means a single anaesthetic, a single recovery period, and the opportunity to harvest septal cartilage for use as graft material in the cosmetic work.
Patients with a confirmed deviated septum causing breathing difficulty, with or without cosmetic concerns. Septoplasty can be performed as a standalone functional procedure or combined with rhinoplasty (septorhinoplasty). It may be partially covered by insurance when performed for functional reasons.
Dr. Buonassisi assesses the septum as part of every rhinoplasty consultation. If a deviation is present and contributing to obstruction, he will discuss whether correction is appropriate and how it fits into the overall surgical plan.
Ultrasonic Piezotome Rhinoplasty
Precise bone reshaping with less trauma, less bruising, and a faster recovery.
The piezotome uses ultrasonic vibration to cut bone with a precision that traditional osteotomes cannot match. The instrument selectively cuts hard tissue (bone) while leaving soft tissue (nerves, vessels, mucosa) intact — reducing the collateral trauma associated with conventional bone work.
Traditional osteotomies involve controlled fractures using a chisel-like instrument. The piezotome achieves the same result with significantly less bruising and swelling — because the surrounding soft tissue is not disrupted in the same way. For patients concerned about downtime, this can make a meaningful difference.
Patients undergoing hump reduction or osteotomies where the anatomy is suitable for the ultrasonic approach. Dr. Buonassisi uses the piezotome selectively — it is not appropriate for every case, and he will advise whether it is the right tool for your anatomy.
The decision to use the piezotome is made based on the bone work required and the patient's anatomy. It is used for osteotomies and dorsal work where precision is important and where minimising bruising is a priority. It does not change the overall surgical approach.
Teen Rhinoplasty
Rhinoplasty for younger patients — considered once facial growth is complete.
Teen rhinoplasty follows the same surgical principles as adult rhinoplasty. The key difference is timing: surgery is only considered once facial growth is complete — typically 17–18 for females and 18–21 for males. Operating before growth is complete risks the result changing as the face continues to develop.
For teenagers who are genuinely distressed by the appearance of their nose, rhinoplasty can have a significant positive impact on confidence and wellbeing. The decision is taken seriously and is never rushed — Dr. Buonassisi requires multiple consultations and parental or guardian involvement throughout.
Younger patients who have completed facial growth, have a clear and stable motivation for surgery, and have the full support and involvement of a parent or guardian. Emotional maturity and realistic expectations are assessed as part of the consultation process.
The consultation process for teen rhinoplasty is more extended than for adult patients. Dr. Buonassisi meets with the patient and their parent or guardian, assesses facial growth, discusses motivations, and ensures that the decision is well-considered before any surgical plan is made.
Find out which technique is right for your anatomy.
Our pre-assessment takes 5–10 minutes and helps Dr. Buonassisi's team understand your goals before your consultation. There is no obligation to proceed.
The procedures within the procedure.
The techniques described in the section above — open, closed, preservation — refer to the overall surgical approach. Within each procedure, Dr. Buonassisi performs a series of individual manoeuvres: precise, targeted steps that address specific areas of the nose. A single rhinoplasty may involve four, five, or more of these manoeuvres working in combination.
Understanding what each manoeuvre does — and why it might be needed — helps patients have a more informed conversation at consultation. The nine entries below cover the most commonly performed manoeuvres in rhinoplasty. Not all will apply to every patient; the specific combination is determined by the anatomy and the goals.
Cephalic Trim
What it is — Removes a measured strip from the cephalic (upper) edge of the lower lateral cartilages — the cartilages that form the tip and alar rims.
Why it matters — Reduces tip bulkiness and width. One of the most commonly performed tip manoeuvres, but requires restraint: over-resection weakens the alar rim and can cause long-term collapse.
Deprojection
What it is — Reduces how far the nasal tip projects forward from the face. Techniques include cartilage scoring, tongue-in-groove setback, or medial crural overlap.
Why it matters — Addresses a nose that protrudes too prominently. Often combined with tip rotation to achieve a more balanced profile.

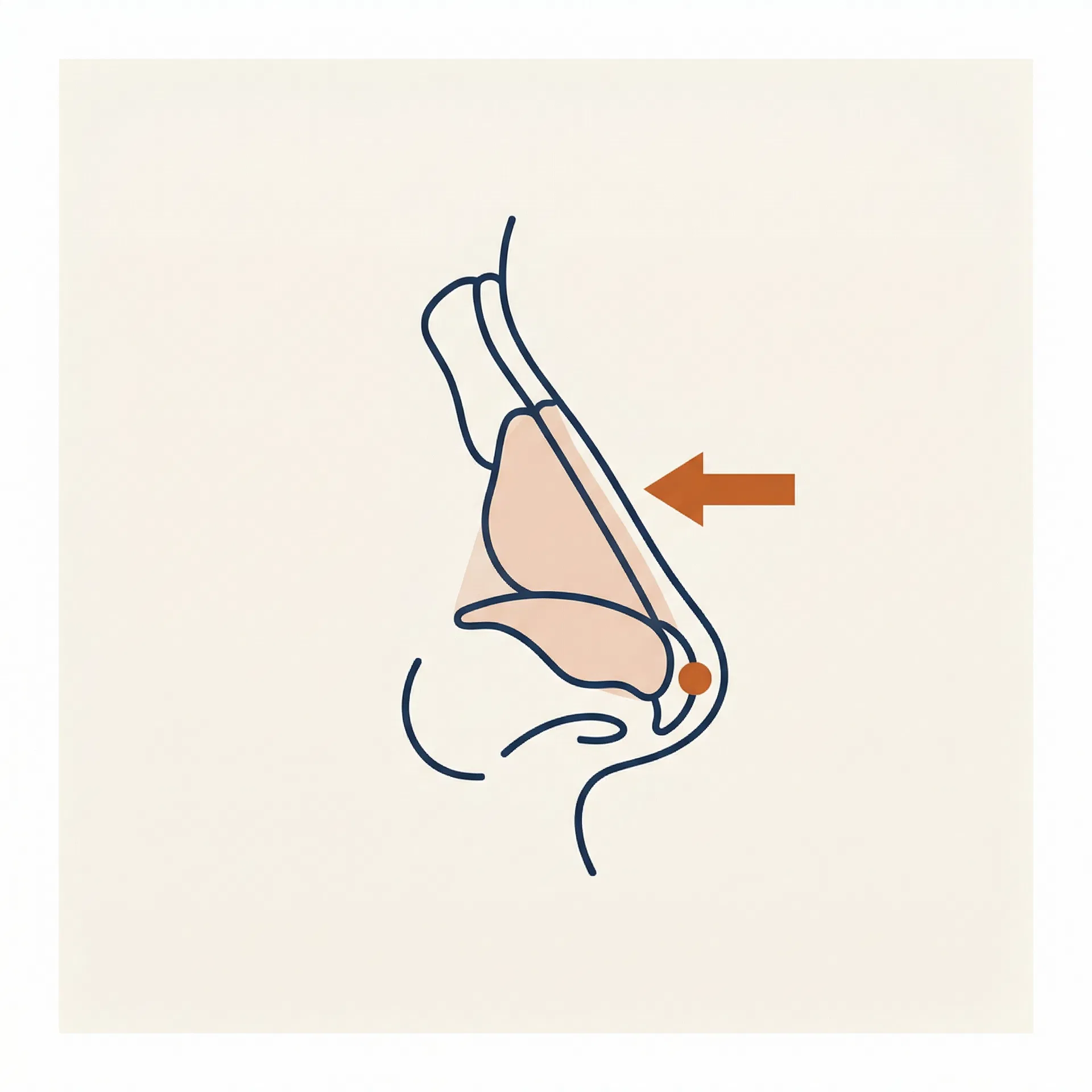
Dorsal Hump Reduction
What it is — Reduces the convex prominence along the nasal bridge — a combination of bone in the upper third and cartilage in the middle third. The hump is either excised (traditional resection) or lowered by letting down the entire dorsum while preserving the native anatomy (preservation approach).
Why it matters — The most commonly requested change in rhinoplasty. Reducing the hump alone is rarely the full picture — the middle vault, tip, and overall profile must all be considered together. Hump reduction without addressing the tip almost always creates a disproportionate result, which is why it is nearly always part of a broader surgical plan.
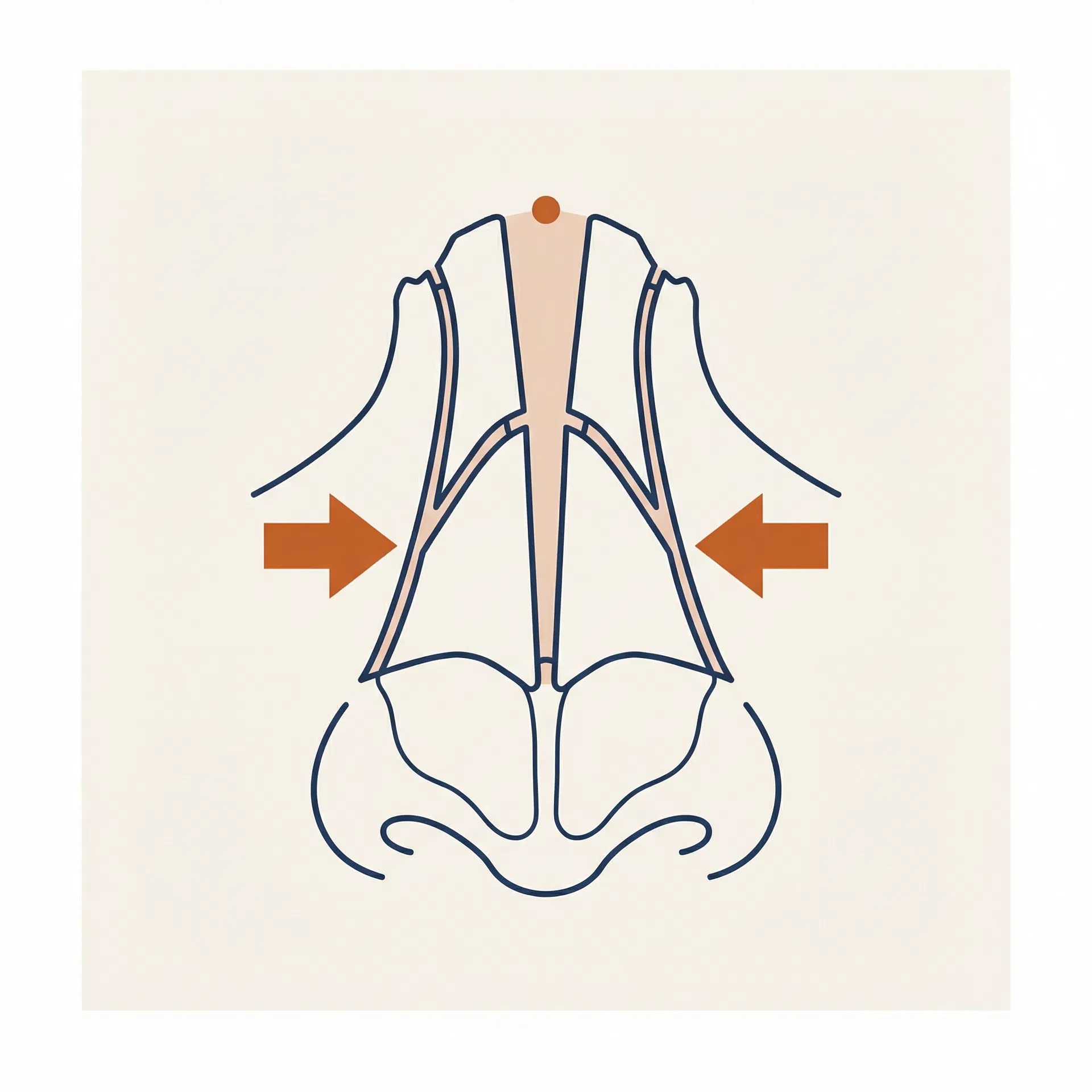
Osteotomy
What it is — Controlled fracture of the nasal bones to narrow the bony vault or close an open roof after hump reduction. Performed through small internal incisions.
Why it matters — After removing a dorsal hump, the nasal bones are left separated — creating an open roof that must be closed by infracturing the bones inward.
Columellar Strut Graft
What it is — A piece of cartilage (usually harvested from the septum) placed between the medial crura of the tip cartilages to create a stable foundation for the tip.
Why it matters — Adds tip support, projection, and definition. Essential in preservation rhinoplasty when tip support has been reduced.

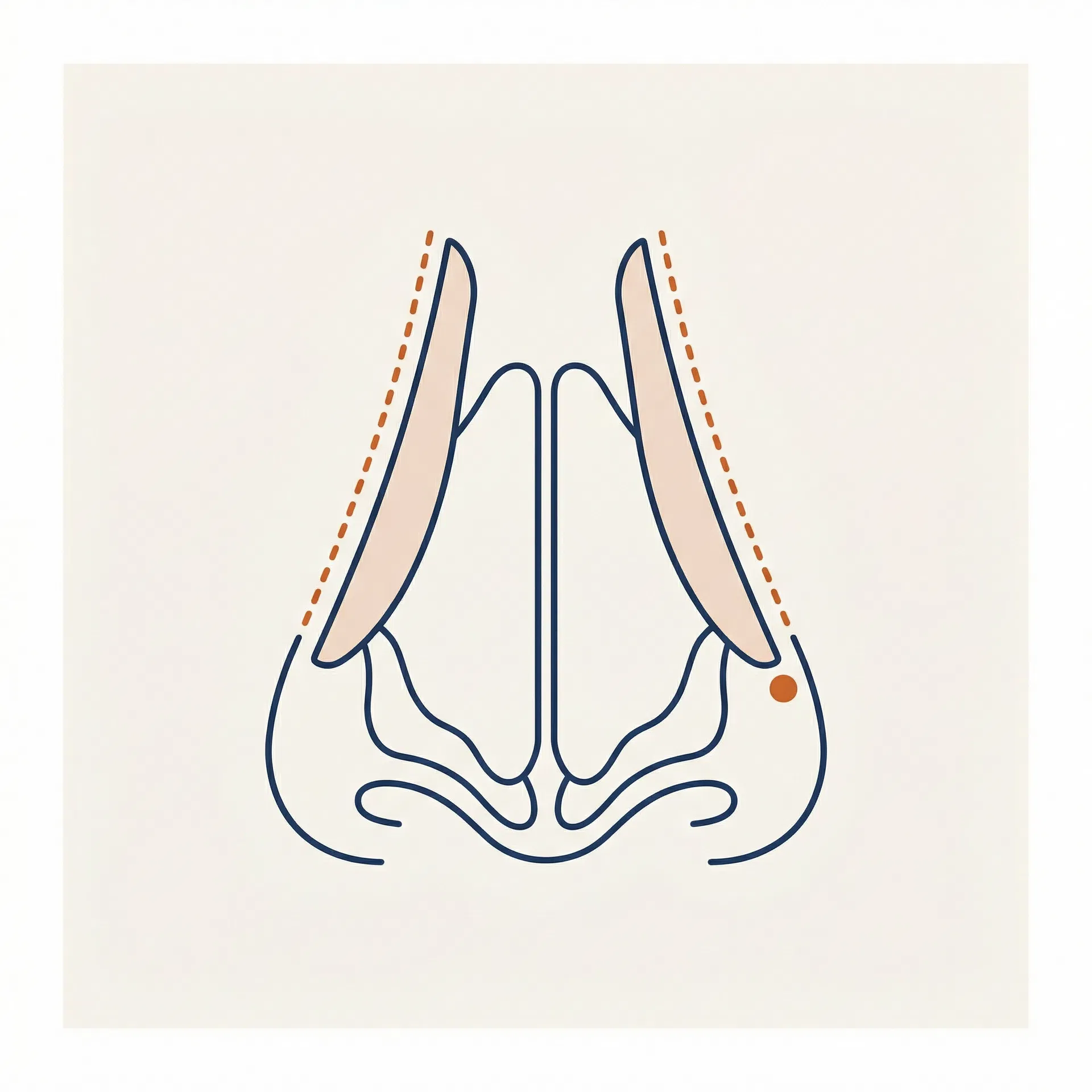
Spreader Grafts
What it is — Thin cartilage grafts placed between the upper lateral cartilages and the septum to widen the middle vault and maintain the internal nasal valve angle.
Why it matters — Prevents the pinched, inverted-V deformity that can occur after aggressive hump reduction. Also used to correct nasal obstruction.
Tip Suture Techniques
What it is — A family of suturing manoeuvres — transdomal, interdomal, and lateral crural mattress sutures — that reshape the tip cartilages without removing tissue.
Why it matters — Allows precise tip refinement with minimal tissue disruption. Preferred over excision in preservation rhinoplasty.

Alar Base Reduction
What it is — Removes a small wedge of tissue at the base of the nostrils (alar wedge excision) or at the sill to narrow the base width or reduce flaring.
Why it matters — Addresses nostrils that are too wide or flare excessively. Often performed as a finishing step after tip and bridge work.
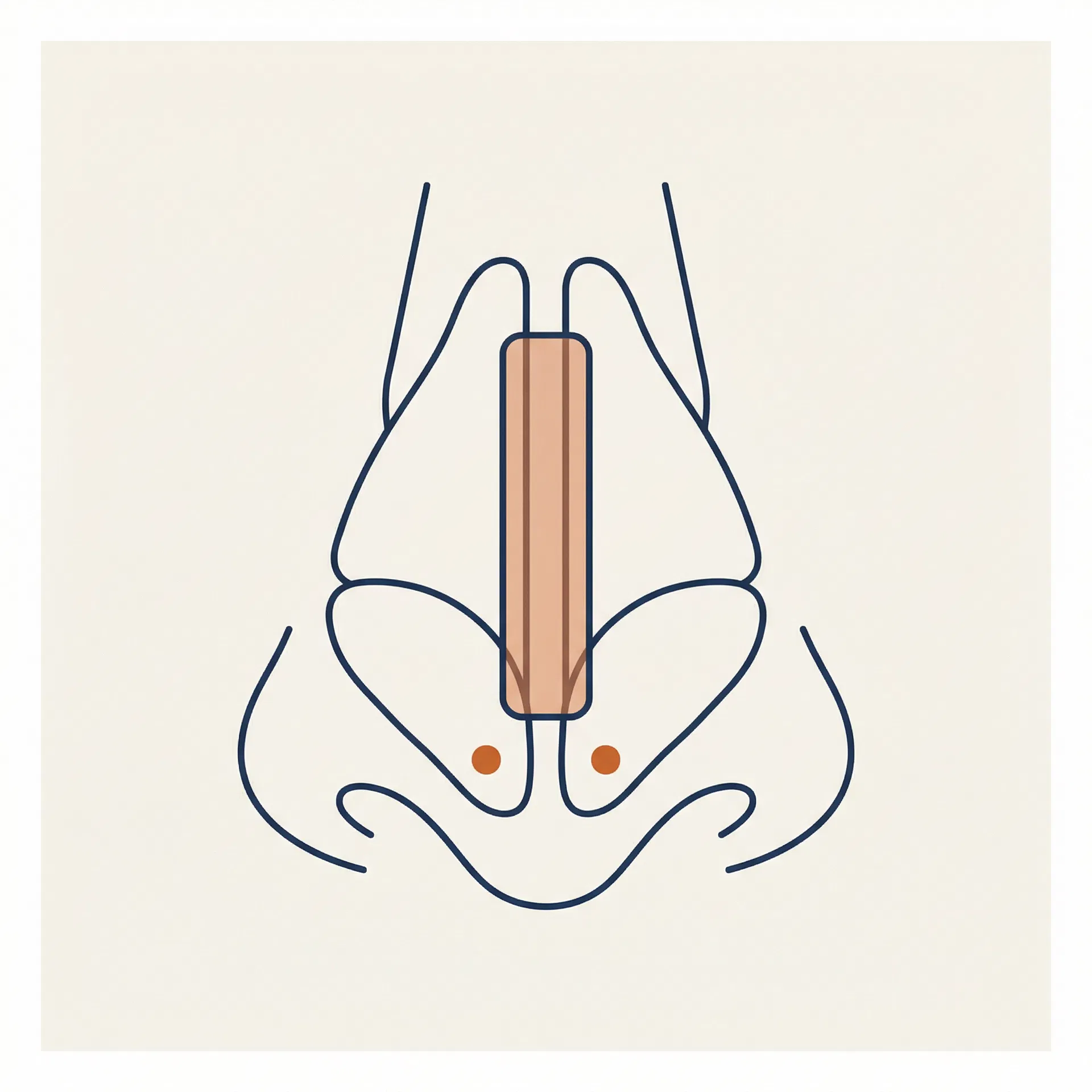
Septoplasty & Cartilage Harvest
What it is — Straightens a deviated septum and harvests cartilage that can be used as graft material for struts, spreaders, or tip grafts elsewhere in the nose.
Why it matters — The septum is the primary donor site for rhinoplasty grafts. Correcting a deviation improves breathing while providing raw material for structural reconstruction.
Rhinion Horn Reduction
What it is — Reduces the bilateral bony prominences on the lateral sides of the nasal bridge near the rhinion — the points where the nasal bones flare outward and create visible widening of the upper bridge.
Why it matters — Distinct from hump reduction, which addresses the dorsal profile line. Rhinion horn reduction narrows the bridge width when viewed from the front, refining the upper third without altering the profile height. Often performed in combination with osteotomies.
Tip Augmentation
What it is — Adds projection, definition, or height to the nasal tip using a cartilage graft — typically a shield graft or cap graft harvested from the septum or ear — placed at the tip to increase its prominence and refine its shape.
Why it matters — Used when the tip lacks projection, appears flat, or needs structural support after other tip manoeuvres. Particularly important in ethnic rhinoplasty and revision cases where native tip cartilage is weak or has been previously altered. Rarely performed in isolation — tip augmentation is almost always part of a broader plan that addresses the bridge and overall balance.
Bridge Augmentation
What it is — Raises the height of the nasal bridge using a cartilage graft (typically diced cartilage wrapped in fascia, or a solid septal/rib graft) or, in some cases, a silicone implant placed along the dorsum.
Why it matters — Addresses a flat or low dorsum — a common goal in ethnic rhinoplasty where patients want to add bridge height while preserving their ethnic identity. The approach is always considered in relation to tip projection and facial proportions; augmenting the bridge without addressing the tip can create an unbalanced result.
Diagrams use the Elevation Mark visual language — the same annotation system applied across all 8 West educational content.
Frequently asked questions about rhinoplasty techniques.
Understand rhinoplasty before your consultation.
Surgeon-authored guides covering technique selection, recovery, candidacy, and what to expect — written for patients who want to make an informed decision.