
Explore Rhinoplasty Types & Goals
Select a technique below to explore how it works, who it suits, and what to expect
1 / 9
Hump Reduction Rhinoplasty
Smoothing the nasal bridge for a refined, balanced profile
Hump reduction rhinoplasty addresses a dorsal hump — the bump on the nasal bridge that can create a convex profile. It is one of the most commonly requested rhinoplasty goals and can be achieved through traditional resection or, increasingly, through preservation rhinoplasty techniques that reshape rather than remove the hump.
What it is
A dorsal hump is a prominence of bone and cartilage along the nasal bridge. Hump reduction lowers this profile line — either by excising the excess tissue (traditional approach) or by letting down the dorsum while preserving the native anatomy (preservation approach). The result is a straighter, more refined bridge that harmonises with the rest of the face.
Why it matters
A prominent nasal hump can dominate the profile and draw attention away from the eyes and lips. Reducing it creates a straighter, more refined bridge and restores facial balance — often with a dramatic improvement in the overall profile without changing the frontal appearance significantly.
Who it’s for
Patients with a visible dorsal hump on profile view who are otherwise satisfied with their tip, nostrils, and frontal appearance. Can be combined with tip work for a full rhinoplasty.
How Dr. Buonassisi decides
Dr. Buonassisi evaluates the hump's composition (bone, cartilage, or both), the strength of the middle vault, and the patient's skin thickness. In consultation, he determines whether a preservation let-down or traditional resection is more appropriate — and whether osteotomies or spreader grafts are needed to close the roof and maintain airway function.
Open vs. Closed vs. Preservation
These three terms are often confused. Open and closed describe the incision location. Preservation describes a surgical philosophy that can be applied through either incision approach.
← Scroll to compare →
| Open Rhinoplasty | Closed Rhinoplasty | Preservation Rhinoplasty | |
|---|---|---|---|
| Incision location | Small external incision at columella | Inside the nostrils only | Either approach, tissue-sparing |
| Visibility for surgeon | Full direct visualisation | Limited indirect access | Variable — philosophy, not incision |
| External scar | Very fine scar, fades over 6–12 months | None | Depends on approach used |
| Best for | Complex cases, revision, tip work | Bridge work, minor refinements | Natural-looking results, hump reduction |
| Swelling duration | Slightly more initial swelling | Slightly less initial swelling | Typically less — less disruption |
| Dr. Buonassisi preference | Primary choice for complex cases | Selected cases | Default philosophy when anatomy allows |
The right approach for you is determined during your consultation with Dr. Buonassisi based on your anatomy and goals.
The Surgical Moves Behind Your Result
Every rhinoplasty is built from a set of precise, individual manoeuvres — each one addressing a specific anatomical detail. A cephalic trim refines the lower lateral cartilages. A columellar strut adds tip support. An osteotomy narrows the bony vault. A deprojection technique reduces how far the nose projects from the face.
These are not a menu you pick from. Dr. Buonassisi determines which combination of manoeuvres is appropriate for your anatomy during the consultation — and sometimes makes intraoperative decisions as the anatomy reveals itself under direct vision. What matters is understanding that your result is the product of many small, deliberate choices, not a single technique applied uniformly.
Cephalic Trim
What it is: Removes a measured strip from the cephalic (upper) edge of the lower lateral cartilages — the cartilages that form the tip and alar rims.
Why it matters: Reduces tip bulkiness and width. One of the most commonly performed tip manoeuvres, but requires restraint: over-resection weakens the alar rim and can cause long-term collapse.

Deprojection
What it is: Reduces how far the nasal tip projects forward from the face. Several techniques exist: cartilage scoring, tongue-in-groove setback, or medial crural overlap.
Why it matters: Addresses a nose that protrudes too prominently. Often combined with tip rotation to achieve a more balanced profile. The technique chosen depends on the degree of projection and the strength of the existing tip support.

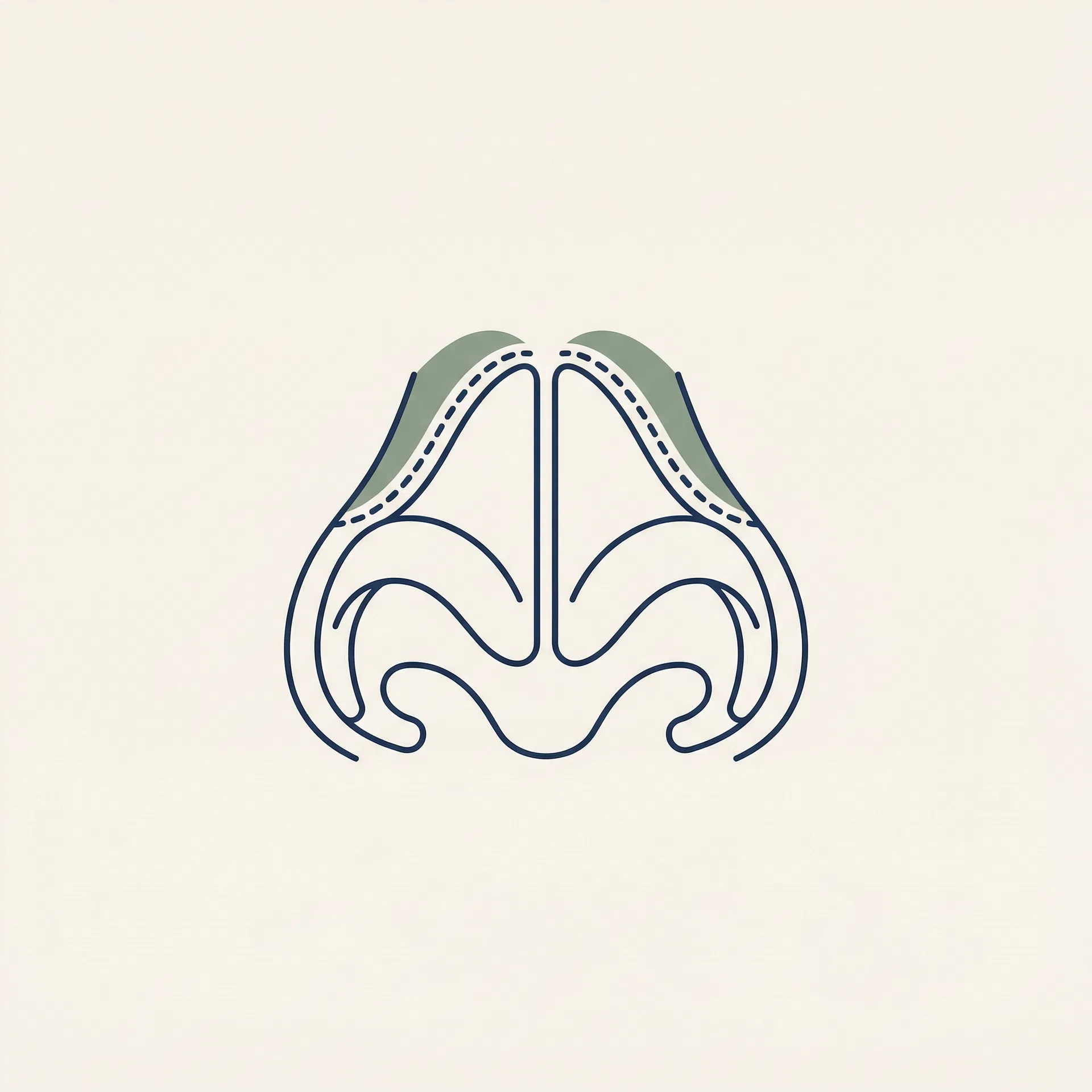
Rhinion Hump Reduction
What it is: Removes or reshapes the prominence at the rhinion — the point where the nasal bones meet the upper lateral cartilages, typically the highest point of the dorsal profile.
Why it matters: The most commonly requested change in rhinoplasty. In preservation rhinoplasty, the hump is lowered by letting down the dorsum rather than excising it — preserving the keystone area and reducing the risk of an open roof deformity.

Osteotomy
What it is: Controlled fracture of the nasal bones to narrow the bony vault or close an open roof after hump reduction. Performed with a fine osteotome through small internal incisions.
Why it matters: After removing a dorsal hump, the nasal bones are left separated — creating an 'open roof' that must be closed by infracturing the bones inward. Also used to straighten a crooked bony nose.
Columellar Strut Graft
What it is: A piece of cartilage (usually harvested from the septum) placed between the medial crura of the tip cartilages to create a stable foundation for the tip.
Why it matters: Adds tip support, projection, and definition. Essential in preservation rhinoplasty when tip support has been reduced, and in ethnic rhinoplasty where native tip support may be limited.
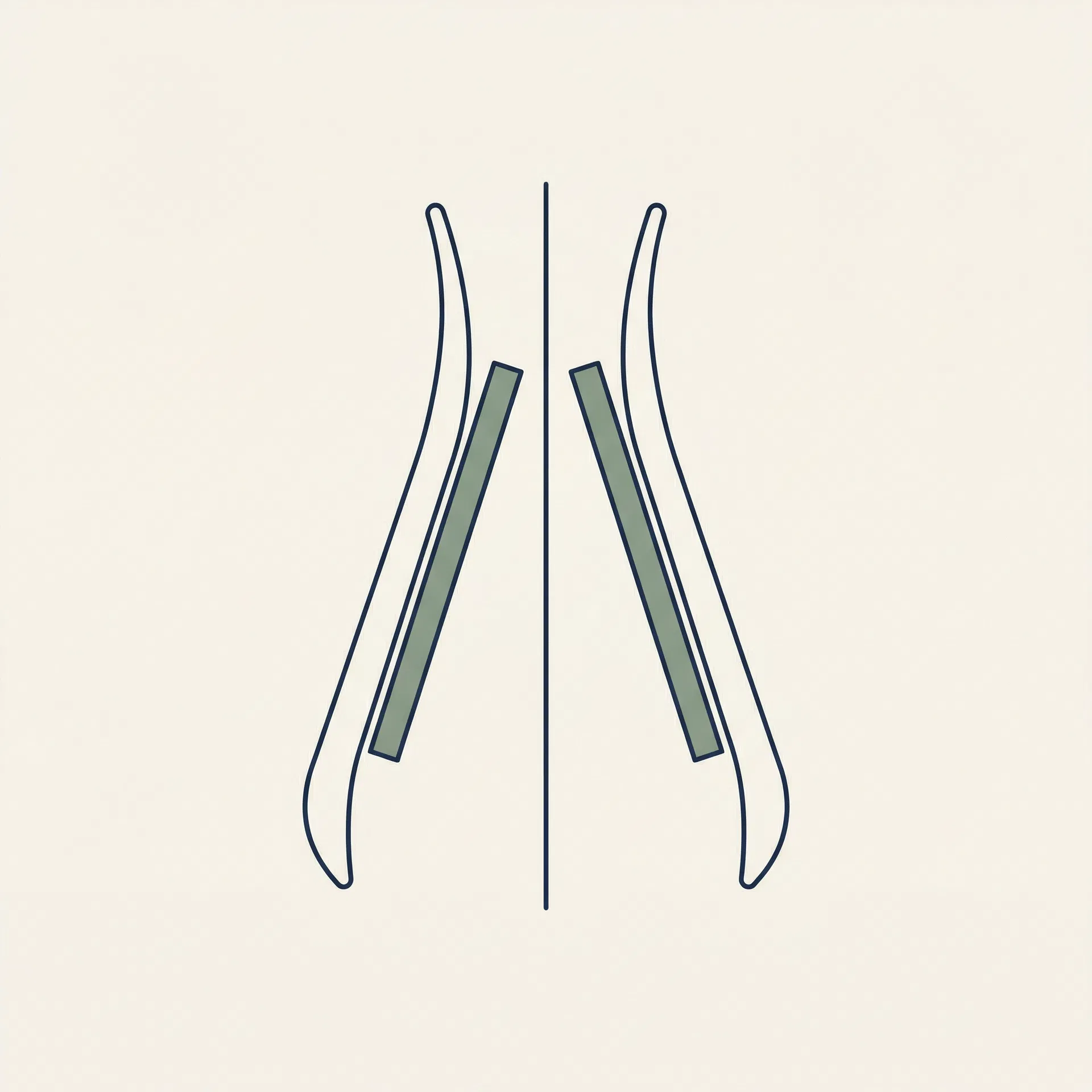
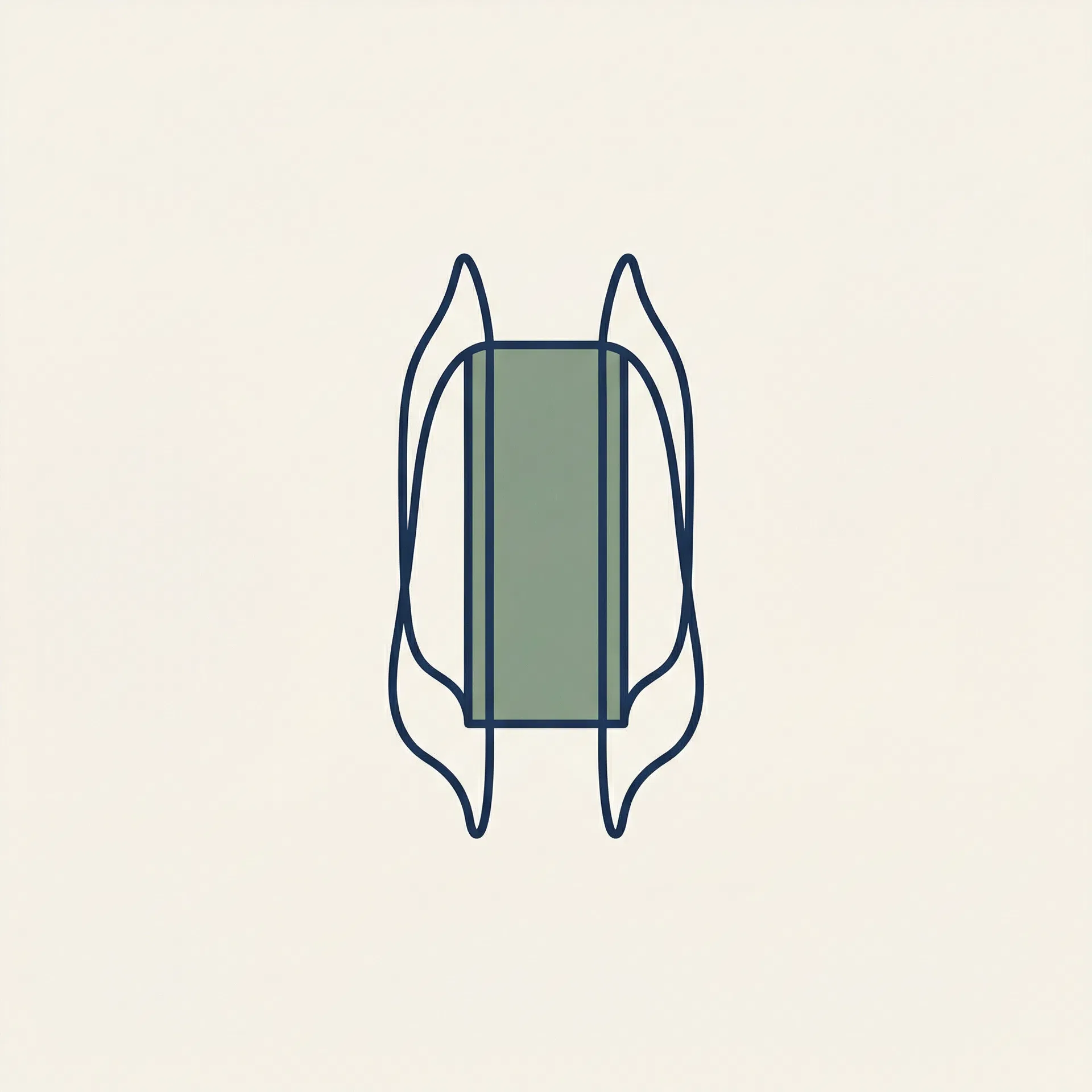
Spreader Grafts
What it is: Thin cartilage grafts placed between the upper lateral cartilages and the septum to widen the middle vault and maintain the internal nasal valve angle.
Why it matters: Prevents the pinched, inverted-V deformity that can occur after aggressive hump reduction. Also used to correct a narrow middle vault that contributes to nasal obstruction.
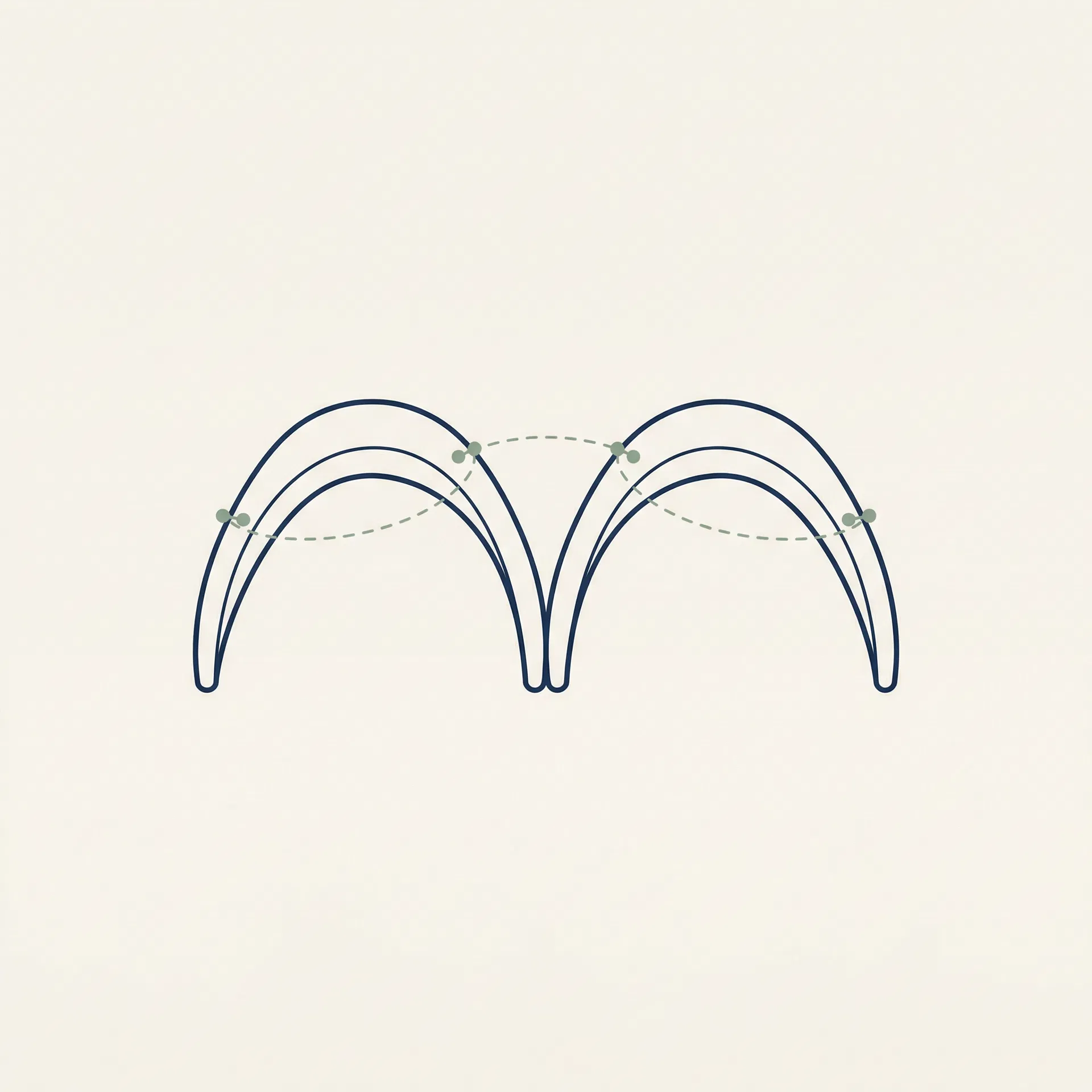
Tip Suture Techniques
What it is: A family of suturing manoeuvres — transdomal, interdomal, and lateral crural mattress sutures — that reshape the tip cartilages without removing tissue.
Why it matters: Allows precise tip refinement with minimal tissue disruption. In preservation rhinoplasty, suture techniques are preferred over excision wherever possible, as they preserve structural integrity and allow for more predictable healing.
Alar Base Reduction
What it is: Removes a small wedge of tissue at the base of the nostrils (alar wedge excision) or at the sill to narrow the base width or reduce flaring.
Why it matters: Addresses nostrils that are too wide or flare excessively. Often performed as a finishing step after tip and bridge work to ensure the base width is proportionate to the new nasal profile.

Septoplasty & Cartilage Harvest
What it is: Straightens a deviated septum and — in the same step — harvests cartilage that can be used as graft material for struts, spreaders, or tip grafts elsewhere in the nose.
Why it matters: The septum is the primary donor site for rhinoplasty grafts. Correcting a deviation improves breathing while simultaneously providing the raw material for structural reconstruction elsewhere in the nose.

Dr. Thomas Buonassisi, MD FRCSC
Board-certified by the American Board of Facial Plastic & Reconstructive Surgery. Over 2,500 rhinoplasty procedures performed since 2008. Specialist in preservation rhinoplasty and complex revision cases.
Technique FAQ
Not sure which technique is right for you?
Tell us your goals and Dr. Buonassisi's team will review your case personally — before you ever step into the clinic.
Strictly confidential · Reviewed by Dr. Buonassisi's team only